In May, Brian was appointed Director of Football at Hibs. After four decades as a professional footballer, manager, and scout, he has also built a strong reputation for delivering motivational talks.Run by Hibs Community Foundation volunteers who have completed the 12-week SAMH Changing Room sessions at Easter Road, ‘Supporting Our Supporters’ is one of the Foundation’s diverse range of community outreach programmes. Held on the last Monday of every month, July’s SOS event was particularly memorable for welcoming Brian McDermott as the guest speaker. The Foundation approached him about the possibility of making a presentation at a future SOS drop-in. Given his day job of managing the pre-season transfers, it was assumed this might occur sometime later in the year. All were delighted when Brian agreed to speak at the July SOS drop-in. On the night, the sizeable audience included HCF volunteers and other regular SOS attendees, current Changing Room participants and SAMH coaches. Read the full article about Brian's visit and motivational talk posted on the website of Hibs Community Foundation.  Credit: Ecosse Photo For a long time, I tried forgetting the psychotic episodes I'd experienced during my 20s. If anyone mentioned my spell in the Andrew Duncan clinic, I'd mention rehab. Not a breakdown. Deciding I wanted to share my story, I requested a copy of my psychiatric case file. These abridged notes detail how the medical staff assessed me during the summer of Madchester and Italia '90, an inpatient in a psych ward suffering a hypomanic episode. Staff names amended for privacy.June 1990 Mark entered the ward following outpatient contact today for assessment. Prescribed chlorpromazine 200 mg nightly and PRN (when required) chlorpromazine. According to Dr Erskine, Mark has the potential of becoming quite unwell. Although initially appearing restless, has seemed to settle into ward: pleasant and obliging on approach. On occasions heard talking when in bedroom alone. Spent time reading, listening to music on Walkman, but posing no management difficulty. Accepted PRN medication. Said he knows when he “needs to be drugged up.” Mentioned to colleague he “did not know you could go up as well as down.” On several instances heard talking to himself, e.g. when walking along the corridor or in the kitchen. Is aware, due to explanation by colleague, of what CLOSE OBSERVATION means. Overnight largactil 100 mg. Slept until 8:30 am. When asked question, anxious to answer, then get on with something else. Thought process jumbled. Is placing his state of health upon the fact the colour red ‘protects’ him from a further breakdown. Largactil 100 mg 12:15. Did not settle till after 02:00. Remains disorganised, dominated by themes of Nazis, World War II, and the colour red he believes can cure him if he touches. PRN dose 100 mg chlorpromazine given 12:20 to clarify thought content. Mark has clear difficulty in concentrating and is unable to settle for any length of time. Did sit still for a short period to do some writing. Speech content remains confused and disordered. Easily distracted during conversation, moving from subject to subject in response to stimuli. Visited by parents today, father expressing concern about their son’s mental state. Out twice today with myself for short walks. Mark‘s conversation focused on his drug abuse and the issue of child abuse. Said, “last time I took drugs was before a church service.” Described his reaction to drug – cannabis? – as a ‘downer’ and this was the usual effect drugs had on him. Talked of the colour red and how touching something red can ward off "bad feelings" and showed me a red object he was holding in his pocket. Mark remains on CLOSE OBSERVATION due to risk of unpredictable behaviour. Restless. Largactil 20 mg given 12:40 with no affect. In and out of bed. Largactil 100 mg given 02:30. Did not sleep till 04:30. Very disorganised both in speech and in behaviour, forgetting where he's put things laid down a moment before. 100mg PRN chlorpromazine dose 07:00 and 09:20 with negligible effect. Duty doctor contacted re. regular regime of chlorpromazine. He came and assessed Mark, prescribed 100mg chlorpromazine tablets 08:00, 13:00, and 18:00, and maintaining present 200mg chlorpromazine @ 22:00 and PRN dose if necessary. Content of speech centring around freemasonry and Nazis, using neologisms frequently and flight of ideas prevalent. Behaviour and speech content bizarre and confused. Mark adopts unusual postures and actions. Unable to settle and concentrate for any length of time - frequently walking the corridor and at times talking to himself. Has changed his shirt a few times this afternoon offering no reason for this. This evening Mark ran out of cigarettes and staff were unable to supply him as he had no cash. Mark became irritable and threatening in voice and manner at prospect of having no cigarettes. Given £1 from ward funds on the understanding this was a loan. Cigarettes bought by fellow patient. Mark has since appeared more settled. On CLOSE OBSERVATION. PRN largactil 100 mg 12:15. Settled 01:00 until 03:15. Bizarre behaviour since. PRN largactil 100 mg 03:40. Did not settle and sleep till 05:15. Behaviour remains very bizarre, posturing continuously, speech content confused and difficult to follow. Extremely restless throughout day, dancing and running about ward, having to be cautioned about over-activity and limits set by staff. Has responded to setting of limits amenably, although due to level of confusion quickly forgets. Giggling inappropriately but appears to be at own thoughts. Kardex chlorpromazine increased and PRN droperidol added to prescription. Mark slept for early part of afternoon and has been drowsy and ‘slowed up’ throughout evening. Still needing limits set on certain behaviours e.g. twice he put his hand in the fish tank to try and catch one. Gesturing a lot when speaking and at times exhibiting bizarre postures e.g. holding left arm out in a twisted position as though he was doing an ‘Egyptian sand-dance,’ also using odd facial grimacing. Visited by mother this evening, out for a 10-minute walk. This evening Mark became increasingly restless, pacing the ward, and intimidating he may hit someone e.g. as Ali Johnston was speaking, Mark held his slipper and gestured he was going to hit her on the back of the head, and going to hit Adrian McCandlish on the bottom. Duty doctor contacted as it was noted in Mark’s notes he had an acute dystonic reaction to droperidol and required IV procyclidine. She wrote him up for chlorpromazine, 200mg PRN (up to 1g in 24 hours.) Thus, 200 mg chlorpromazine PRN given at 20:20. Dr Erskine contacted IPCU and advised them of Mark’s mental state in case he needs to be transferred during the night. M Wonacutt (acting nursing officer) informed to ensure adequate nursing cover tonight and to inform her of Mark’s mental state at present. CLOSE OBSERVATION continued. Settled and slept after 22:00 medication. Given PRN procyclidine as advised by medical staff. Behaviour becoming increasingly inappropriate i.e. head held close to a bedroom door, peering around doorframes, hunching down in corridor, giggling, content of speech inappropriate - given PRN chlorpromazine as prescribed. Said his friends’ voices “in my head” are calling him different surnames, but don’t say anything else. Claims he says he has control over voices, which he experiences all the time. Went for a short walk around hospital grounds with medical student. Continues to exhibit bizarre behaviour, posturing and walking strangely down corridor. Continuously overactive, dancing at times, continues to misrepresent people, and it’s difficult to follow his thought processes. Some disinhibition displayed. Enjoyed sitting out on the verandah during the afternoon. Restless but more appropriate in behaviour. Slept from midnight. Continues to be overactive and carries out ritualist gestures. A little grandiose in speech, but not as pressured and no flight of ideas. Overall conversation appropriate and concentration improved, though occasionally appears restless, wandering about ward. Spending time on verandah with Ward 1 patients and watching TV. Visited by a friend this afternoon and family later in the evening. Remains on CLOSE OBSERVATION. Slept until 07:30. On rising, appeared restless, often gesticulating. Said he’s hearing voices but would not discuss content. Often appears preoccupied but unwilling to discuss. PRN chlorpromazine had minimal effect. On one occasion was about to go to shops with patient from Ward 1 without informing nurses. Has been advised that due to his present condition must have a nurse escort if going out of ward. Appears to be interacting well with fellow patients. Settled in afternoon. Concentration level fluctuations most of the shift. Restless and admitting to auditory hallucinations. PRN chlorpromazine 200 mg given 01:30 with no effect until 3:30. Constantly active all morning, walking about in and around ward. Conversation often inappropriate. Gesticulating. Appears to be eating and drinking a great deal. Mixing with fellow patients but unable to settle for any length of time, becoming irritable on occasion. His whereabouts and activities need to be constantly monitored. Tending to lay his belongings in a variety of places around the ward. Concentration poor. PRN chlorpromazine given as per Kardex has minimal effect, if any. Dr Erskine suggested chlorpromazine PRN be given, if needed. Has been restless this afternoon. Encouraged to rest on the bed after lunch for an hour and before tea for half an hour. Speech in the main appropriate, though at times has been seen to gesticulate facially and with limbs in a bizarre manner. Asking at times he can go out on his own, explained that due to CLOSE OBSERVATION he cannot. Managed out for a while this evening with his sister and a friend. Mark is eating large amounts of food, but to no ill affect. Restless and inappropriate conversation, laughing and muttering to himself. PRN chlorpromazine 200 mg at 23:30. Eventually slept from around 02:00. Remains on CLOSE OBSERVATION due to inappropriate behaviour. Rather disorganised this morning needing close observation for unpredictable behaviour. Out for a walk to Morningside with occupational nurse. Mark needed much supervision due to his disorganisation. Needed PRN chlorpromazine 200 mg at 11:50 for restlessness and apparent response to auditory hallucinations. Has been reasonably settled, speech content in the main has been appropriate. Mark has managed a short sleep this evening. Went out for a short while with a friend and later with his sister. Appreciates getting outside. Still requires CLOSE OBSERVATION for unpredictable behaviour. He also has been rather disorganised and forgetful - left running tap with plug in the basin at which he seemed embarrassed. Fairly settled evening although appeared confused on occasion and quite tired. Retired at 23:30 and appears to have slept well overnight. Remains on CLOSE OBSERVATION due to unpredictable behaviour. Very impatient awaiting visit to shop for cigarettes. Quite appropriate when out, and although overactive and confused at times, certainly appears improved and has said so himself. Restless at times, flitting from one activity to another showing poor concentration. Also complaining of being bored but has made a friendship with a Ward 1 patient. Speech content in the main has been appropriate and he says he is pleased with the apparent improvement in his mental state. Remain somewhat disorganised, sometimes forgetting where he has left things. Out for a short while with his parents this evening. Remains on CLOSE OBSERVATION. PRN largactil 200 mg, procyclidine 5 mg given 12:30, settled and slept. Spent most of morning wondering around the ward, needing limits set on behaviour. Rather more appropriate in speech. Has appear reasonably settled throughout the afternoon, not requiring PRN medication. At times forgetful as to where he has left things such as his coat. Frequently asking to get out for fresh air on his own, explained not possible due to CLOSE OBSERVATION. PRN largactil 200 mg given 12:30. Settled 03:30. Still needing limits set on certain behaviours e.g. twice he put his hand in the fish tank to try and catch one. Very disorganised and pacing constantly along the ward. Out for a spell on verandah. Remains on CLOSE OBSERVATION and disorganised manners. Communicating inappropriately. Slightly anxious about commencement of his treatment. Mark told he can go for unaccompanied walks around the grounds, but not to shops as behaviour remains unpredictable. Mark appears to have had a reasonably settled morning. Reduced to STANDARD OBSERVATION, although requires to be accompanied outside of hospital grounds. Remains disorganised and confused at times, although overall more settled. Remains muddled overnight. Unable to make decisions. Slept until 05:00 and has been restless since. Noted to be missing from ward at approximately 10:30, not having inform staff he was going out. Search made and not found. Received phone call from his father at 11:30 to say Mark was at a friend’s house. Dad brought him back. Appeared very muddled and confused, distracted, denying he had been asked not to leave the ward without informing nursing staff. Returned to CLOSE OBSERVATION and must be accompanied by a nurse. Mark appeared to accept this in an abstracted manner. Restless when he had no cigarettes - this remedied as soon as he bought some from Morningside (accompanied by a nurse.) Retired 23:00. Weekend pass withheld due to Mark’s unpredictable behaviour. Is now to receive another 5 mg procyclidine 18:00. Slept until 07:30. Said he felt better for having had a long sleep. On the whole, has appeared generally settled at times. Had a routine ECG as he has commenced lithium - yet to be seen by medical staff but appears normal. Went out with mum and dad for a run in the car and on return to ward appeared much more settled, although confused at times. Has been talking about going to the pictures with his sister tomorrow. Remains on CLOSE OBSERVATION. Settled and appropriate during evening. Settled approximately 11:30 and slept well since. At times easily distracted. Concentration poor. Enjoyed trip to pictures with sister. Collected by parents. Mrs Fleming thought Mark has proved quite a lot over the past couple of days. CLOSE OBSERVATION continued. Settled and slept. Pottered around the ward and very supportive to another patient who was distressed. Much more settled this afternoon. Chatting away. Gone out for the afternoon and evening with a sister. Due to return at 19:30. CLOSE OBSERVATION continued. Appropriate speech on behavioural approach me to talk about lithium and his ‘illness.’ Mark appears to have insight into his need to take time off from work prior to recommencement. Out with a sister and a friend this evening settled at time of report. Out to shops with friend Emma for half an hour and now on STANDARD OBSERVATION. Out of ward from time to time for short periods and telling staff firstly where he is going. Has spent time with visitors and appears settled. Looking forward to pass Friday to Sunday. Out with his parents for the afternoon and evening for his mother’s birthday party - due back in ward 20:30. Returned to bedroom 23:00. Slept well. Quite bright in the morning, out to Morningside with fellow patient, EmmA. Out with parents for afternoon and evening - has 18:00 medication, due back at 20:30. Sat watching TV retired to bed around 11 pm. Slept well, up at 05:00. It was discussed and agreed Mark can go out on a day pass from 10:00 to 20:45 tomorrow with his family. Also discussed chlorpromazine will be stopped on discharge, gradually, but lithium maintained, and importance of lithium explained. A good morning, out to Morningside with Emma, says he feels “much better now” and realises the odd thoughts he had on admission were not real but down to his illness. Up early this morning, appeared settled. Is out for the day with family, due to return around 20:00, supplied with medication. Continues to tolerate lithium therapy. Pass agreed Friday to Sunday, due back at 20:00. Watched TV all evening and slept. A quiet morning, out to Morningside with Emma. Collected by his dad this afternoon. Mark has gone on a pass until Sunday evening. Return from pass at handover. Settled on ward and slept well. Has gone out with mum and dad for the afternoon, due to return by 21:00. Dad has appointment to see Dr Erskine tomorrow at 14:00. Out with parents this afternoon, due back on the ward at 20:30. Present on ward at changeover. Improvement maintained, slept well, up for breakfast. Spent much of the morning out of the ward. Out for the afternoon and evening with friends, due back 22:00. Returned to the ward and is asking if he can have permission to go for a pub lunch with his parents tomorrow as it is his birthday. Procyclidine discontinued as it no longer deemed necessary. Mark spoke with Dr Erskine about his discharge. Advised to take 3-4 weeks off work to convalesce. Is planning to visit the office with his father to make contact again. Going out for a bar lunch today with his parents for his birthday. Kardex for discharge, bright and settled around the ward. Out of the ward all afternoon, due to return at 21:30. Quiet and appropriate around the ward. Making plans for discharge this afternoon. Went home at 14:15. In June 1990, I was admitted to Ward 1A of the Royal Ed, my bipolar swings having soared into hypomania. My family had been increasingly concerned by my erratic behaviour; a consultation with a psychiatrist confirmed their fears I was broaching mania, at the dangerous top end of the bipolar mood scale. The graph produced by Bipolar UK (below) is not meant to be definitive, but is an indicator of possible behaviours. A copy can be downloaded from the Bipolar UK website and used as a 'mood diary' for anyone with bipolar tendencies "to help keep track of your moods and to help you spot your patterns, triggers and any early warning signs of a relapse." 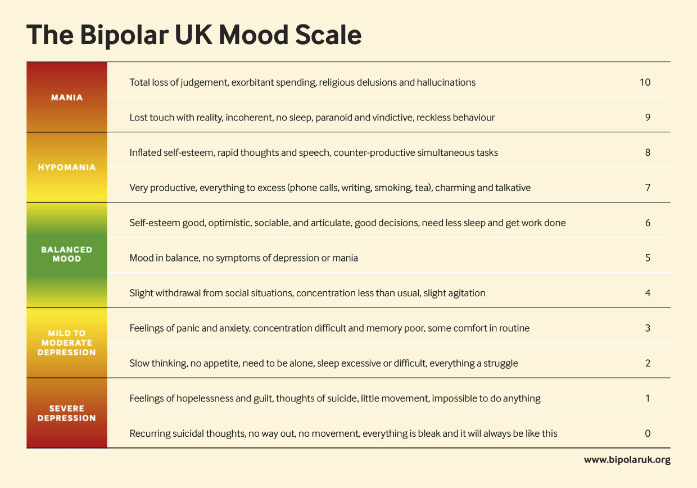 Abridged excerpts from my Royal Edinburgh Hospital records. 15-17 June.Thursday 14/6 - Friday 15/6 Close observation continued. Restless. Medication at 12:30 AM. Largactil 100 mg. Settled and slept. Friday 15/6 Slept until 8:30 AM. Slightly restless on occasion. When asked a question appears anxious to answer then get on with something else. Appears to be interacting reasonably well with fellow patients. Urine specimen to be obtained for clinical chemistry drug scan. PM Still appears disorganised at times. Placing his state of health upon the fact that he's wearing the colour red and is therefore protected from a further breakdown. Thought process appeared jumbled at times. Close observation continued. Restless. Largactil 100 mg given 12:15 AM. Did not settle till after 2:00 AM. Saturday 16/6 Remains rather disorganised, thought content jumbled at times and dominated by themes of WWII/Nazis and the colour red he believes can cure him if he touches it. PRN 100 mg chlorpromazine given 12:20 PM in order to clarify his thought content. PM Mark appears to have had a reasonably settled day, despite having clear difficulty in concentrating and being unable to sit still for any length of time. Did however sit for a period to do some writing. Speech content remains confused and disordered. During conversation becomes easily distracted, moving from subject to subject in response to stimuli. Visited by parents, expressing further concern about son's mental health. Out 2 x escorted by myself for short walks. Mark's conversation focussed mainly on drug abuse and the issue of child abuse. Said the last time he took drugs was 10/6/90 following a church service. Described his reaction to the drug (cannabis) as 'a downer.' Talked also of the colour red and how touching something red can ward off bad feelings and showed me a red object he was holding in his pocket. Mark remains on close observation due to risk of unpredictable behaviour. Saturday 16/6 - Sunday 17/6 Close observation continued. Restless. Largactil 200 mg given 12:40 AM with no effect. Restless. In and out of bed. Largactil 100 mg given 02:30 AM. Did not sleep until 04:30 AM. NOTES: PRN: pro re nata. Medication issued when required, over and above daily dosage. Largactil: a brand name for chlorpromazine, an anti-psychotic drug commonly used in the treatment of schizophrenia, bipolar disorder, attention deficit hyperactivity disorder, and other conditions. One property of this medication is that it can work as a 'dopamine antagonist,' blocking dopamine from activating certain types of cells in your brain and body, slowing down the activity those cells control. Side-effects include dry mouth, movement problems, low blood pressure upon standing, sleepiness, and increased weight. Patients have nicknamed chlorpromazine 'the chemical straitjacket.' In one chapter of my mental health memoir, 1976 - Growing Up Bipolar, entitled 'Pills 'N' Thrills And Straitjackets,' I paint a graphic picture of what happened when I was an outpatient, mixed chlorpromazine tablets with copious alcohol, then headed into a Lothian Road nightclub, The Amphitheatre. 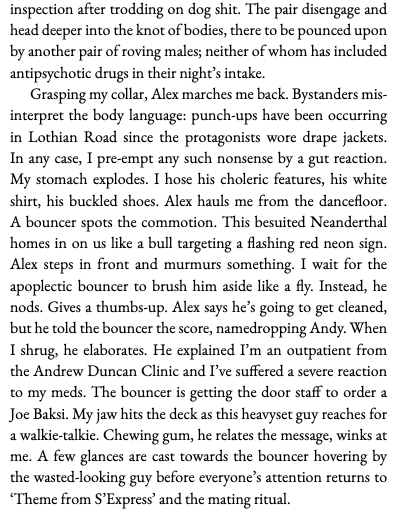 Thought process: my obsession with the colour red goes back to the time I crashed to zero on the bipolar scale in 1987. In the back of an ambulance, delusions whirling, I spotted a red light. A brainwave: saying the word ‘red’ aloud would wake me from what I assumed was a weird, horrific nightmare. But the paramedics had injected me with a strong sedative, so I couldn’t even open my mouth, far less try using some magical password.
Heading towards 10 in the summer of 1990, when I felt my hypomania rising, my deluded imagination thought touching anything red would bring me back down. On one occasion I discovered a Lego set in the ward. Mind racing, I started using the bricks to construct the flags of any of the countries in the current World Cup tournament containing red: Austria, Romania, Spain, Costa Rica (who, ignominiously, beat Scotland 1-0), England, and West Germany (the eventual winners!) 
After coming across a call for artists/writers to submit a proposal for this year's Creative Health Symposium, hosted at the Byre Theatre, St Andrews, I was delighted when my 'pitch' for a 10-minute talk was accepted.  The Symposium comprised a series of events showcasing how writers, musicians, and artists are engaging with audiences under the overarching theme, Creative Health. This was organised by SHARE (Sciences, Humanities and Arts Research Exchange), RCS Innovation Studios, and the Graduate School for Interdisciplinary Studies at the University of St Andrews. Described as an 'in-person, interdisciplinary symposium on the theme of Creative Health, with presenters, performers, and participants from a broad array of artistic, scientific, medical and humanities disciplines,' this symposium was held in the Byre Theatre's conference suite. The event was free, with lunch and refreshments provided. The speakers covered a diverse array of creative topics, relating how they apply writing, music, and even computer gaming to engage with individuals and communities, especially those who are disadvantaged in any way. These ranged from using music directly, memoir writing (cough), poster design, touch-screen information, and many other creative processes. The invited speakers included Claire Ruckert, Ines Jentzsch and Rachel Drury, Mary Black, Thulani Rachia, Amadu Khan, Emily Davis and Beth Whiteside, Catherine King, Kai DurkinClaire Ruckert, Ines Jentzsch and Rachel Drury, Mary Black, Thulani Rachia, Amadu Khan, Emily Davis and Beth Whiteside, Catherine King, Kai Durkin, and myself. After the morning session of 10-minute talks (the most nerve-wracking moments of which were the facilitators brandishing A4 deadline sheets indicating '2-minutes remaining'!), the attendees broke off into small groups for thematic conversations. Posters designed to illustrate the core theme were shared. After lunch there were 15-minute creative presentations (film/music/performance/participatory) featuring Sarah Hopfinger (dance, disability), Kathryn Steven + the poet-doctors (medicine, writing), Ellen Thomson and Kally Lloyd-Jones, John de Simone, Sonia Allori (in collaboration with Laura Gonzalez), Wan Sheng Kenneth Tay, Lynsey Brown, Kenneth Boyd, and Andrew Williams. The inspirational day concluded with a workshop, and optional art/craft activities. My pitch:What my 10-minute walk will focus on: TITLE: MIND GAMES AND MOOD MUSIC Aged 25, I was diagnosed bipolar. At my lowest ebb, I considered suicide and spent time in a locked psych ward. At my highest, I was existing on a few hours’ sleep, binge drinking and churning out bestselling (never completed) novels. I’ve played in bands since the late 70s, eventually recording a BBC Radio 1 session. My passion for music has been crucial to my recovery and ongoing wellbeing. A long-lapsed love in my life, Hibernian FC, has been reignited, especially since joining an outreach programme for fans with lived mental health issues organised by the Scottish Association for Mental Health. This group has evolved, collaborating with similar initiatives in clubs across Scotland, and we’re busy rolling out our self-help hub to the wider community. I’ve also written a memoir about my experiences which I’ve spoken about in schools, community groups, and prisons. A question: “Music and sport have massive potential for inspiring positivity. With suicide remaining the biggest killer of males under 45 how can we tap into these communal passions to promote better health?” A work to share: Readings from my memoir: 1976 – Growing Up Bipolar. My 10-minute talk (cut much shorter by time constraints and inadvertently pressing some random button on the iPad causing my script to vanish for long seconds. While the audience waited. And the camera recording the event for posterity kept rolling... )Good morning. My name is Mark Fleming, and I’m delighted to have been invited along to talk to you about my lived experience of illness and recovery from a mental health condition. I begin by quoting a familiar statistic. Around one in four people are estimated to be affected by mental health problems in Scotland in any one year. Does this imply that three in every four people coast through their days, unduly affected by stress? Of course not. These figures merely illustrate those individuals who have taken the step to admit their problems and seek the medical counsel that has allowed their condition to be classified, whether that’s an anxiety disorder, depression, bipolar disorder, post-traumatic stress disorder, schizophrenia, an eating disorder, disruptive behaviour, or various other disorders. But since a cardinal symptom of having a mental health issue is often denial, putting on a brave face that masks the truth, it would be fair to describe one-in-four as the metaphoric tip of the iceberg. Factors impacting mental health We all have mental health, but such is the complexity and fragility of the human mind, it is all too easily derailed by one or more of a wide range of factors.
The bipolar scale I was diagnosed with manic depression in 1987, a condition now referred to as bipolar, and characterised by mood swings, from extreme highs (mania) to extreme lows (depression). Like the majority of patients who receive this diagnosis, I was a young man (in my mid-20s at the time). Bipolar has often been characterised by a scale running from 0 to 10. This scale is certainly not meant to be definitive in any way, but it does serve a purpose in indicating possible behaviours, many of which will strike a chord with anyone who has lived with a bipolar condition. The inference is the majority of people tend to live their lives around a middle zone, between five and six, their moods balanced. This will dip according to certain situations as everyone will go through challenging events such as family bereavement, relationship breakups, job loss, adverse medical diagnoses, or any number of other exacerbating influences that can have a negative effect. Conversely, lives can be invigorated by positives: getting married, childbirth, holidays, job promotions. Beyond this Meridian, individuals can slide into mild to moderate depression. On that bipolar scale, this would be indicated by lapsing into four. Three. Feelings of panic and anxiety, difficulty with concentration, poor memory. Down to two. Slow thinking. Lethargy. A lack of appetite. A desire for solitude. Erratic sleep patterns, either excessive sleeping or insomnia. Overwhelming notions that everything has become a struggle. This can sink down to one: severe depression, feelings of hopelessness and guilt, isolation becoming agoraphobia. Finding it impossible to do anything. When bipolar hits into zero, the sufferer might be plagued by suicidal thoughts, the notion there's no way out and everything is bleak and it will always be this way. At the other end of this scale is hypomania, when a balanced mood veers into seven or eight. Becoming extremely productive, doing everything to excess whether that's using the phone or other mobile gadgets, writing, smoking, drinking alcohol or taking recreational drugs. A person can become talkative and extremely charming. Have an inflated self-esteem, characterised by rapid thoughts and speech. These flights of fancy might seem fill an individual with optimism and a sense that they could achieve anything, undertaking a variety of tasks simultaneously. But the result of attempting to spin too many proverbial plates is inevitably counterproductive. Many diagnosed with bipolar are prepared to live with the consequences of swerving into hypomania, because of the periods of extreme creativity this can inspire. Unfortunately, this elevated sense of excitement is delusional, and hypomania will only last for short bursts. When this unnatural euphoria becomes prolonged – right up to nine and 10 on the bipolar scale, it is classified as mania. Losing touch with reality. Becoming incoherent. Very little sleep, reckless behaviour, religious delusions, hallucinations. Sectioned in 1987 In 1987 I was diagnosed with a serious mental health condition, initially described as a schizophrenic episode. I was working in a clerical job involving long hours with compulsory overtime. Still in my mid 20s, I assumed the best way to counteract this mundane day-to-day existence would be to continue partying as I had when I've been a Napier University student up until the previous summer. My weekends consisted of 9 am starts both Saturday and Sunday while remaining a hedonistic clubber who spent his leisure time drinking in Buster Browns nightclub until last orders at 3 am. When I eventually hit a metaphoric wall, my health unravelled rapidly. I became introverted, couldn't see a future. Withdrawing from my social circle, I was signed off work with what was euphemistically referred to as stress. Hiding away in my bedroom, I refused to speak to friends who phoned up to ask how I was getting on. I approached the stage where any sort of professional intervention would have been meaningless. My parents were seriously concerned about my erratic behaviour and insisted I see my GP. But with my delusions hurtling out of control, I was convinced my GP wasn't a doctor at all but a football hooligan masquerading as a health professional. When he prescribed antidepressant tablets, my mind had become so unhinged I assumed taking them each night was a form of prolonged euthanasia. I thought my parents and this quack had conspired to poison me. Things came to a head one night when I became so delusional I assumed the only way to make myself better was to knock myself unconscious – a drastic form of resetting. Like switching a computer off and on again. I headbutted my bedroom wall. All this did was give me concussion. My parents burst into the room alarmed at the mysterious thuds emanating from my room. My dad was forced to sit on me to prevent me from self-harming, while my mum dialled 999 and requested an ambulance. Because this was a violent incident, the ambulance arrived with a police escort. I was secured in a straitjacket and taken to the intensive psychiatric care unit at the Royal Edinburgh Hospital. Sometime later, I was formally sectioned. There followed a lengthy period of rehabilitation involving intense medication and occupational therapy. I was eventually granted weekend passes and after being discharged a painstaking readjustment began. Many months later I got a job as an administrative assistant in the Scottish government, although my position was probational due to my health condition. Hypomania in 1990 On that one to 10 scale I was firmly in the middle section, and this persisted for another three years until the bipolar planets aligned again and I started creeping further up the scale. I’d left home for the first time, became a lodger in my sister's flat. This meant I had so much more freedom to go out socialising. I just started a new job in a different department in what was then called the Scottish Office, making friends. My social life was buzzing but I found it difficult to focus on anything, my workload or leisure pursuits. I had fantastical notions about writing a bestselling novel or collection of short stories to add to the ones I'd had published over the years. My turbulent imagination encroaching on 10 (full-blown mania), I was hospitalised again. The outcome of this was being placed on long term antipsychotic medication for a period of almost 30 years. Touch wood, I haven't sunk/soared into the lower or upper ends of that bipolar scale since then, but have finally come off lithium. Lithium is a drug that can certainly improve mental outlook by suppressing extreme emotions, but it also has notable side effects, particularly the way it can impair organ functions: especially the thyroid gland, the kidneys, and the liver. Whilst I was on lithium I was monitored every three months by getting my blood checked on my local GP's. However my mental outlook was never monitored in the same way. Coming off lithium, music, and walking Eventually I made an appointment myself at an outpatients clinic in Edinburgh and requested coming off lithium. The psychiatrist referred to my file and seemed perplexed - no one else on her books had been a lithium patient for so long. Since coming off the drug I've tried filling my life with other positives. I've always been really into music. Aged 17, back in the late 70s, I joined my first punk band. Long before experiencing the manic depression of my mid 20s, I was playing gigs regularly and my band featured on Radio One. Music has always been extremely important to me, and the element most crucial in lifting me from severe depression in 1987 wasn't medication or occupational therapy: it was my sister bringing my Walkman during a ward visit. I also love the great outdoors. Living in Portobello, next to the Firth of Forth, there are fabulous walks nearby. This is another tremendous way of recharging the batteries. During lockdown, I started aiming to do X thousand steps daily, going to different locations with my headphones on and absorbing uplifting playlists. BrainBomb, a semi-autobiographical novel In 2009 I published a semi-autobiographical novel based on my time in the intensive psychiatric care unit, entitled Brain Bomb. Because of the manic delusions and heavy medication, so much of what I’d been through was a mystery. I made up for the extensive blanks by injecting the narrative with fantastical sequences, partially inspired by the time-travelling adventures of Billy Pilgrim in Kurt Vonnegut’s Slaughterhouse 5. Then I had a lightbulb moment. Like any mental health story, maximum impact and poignancy would be achieved if I told the truth. I applied for my case file from the Scottish NHS. This opened a window into my breakdowns, from painstakingly recorded observations from nursing staff in the ICPU, to recommendations for treatment by various psychiatrists, including, if the pills were unsuccessful, electroconvulsive therapy. What I was then able to write was a memoir. Flashback to 1976 - an incident triggers a slow-burning depression I've described how my mental health dipped in the summer of 1987. But mental health can be triggered by all those factors I've mentioned, including childhood trauma. I believe my depression didn’t suddenly erupt over a few months when I was 25. My inexorable slide began much further back, instigated by an incident during the long, hot summer of 1976. When I was 13, at a Sunday school picnic, I was abused by a predatory pedophile male. I became extremely withdrawn. Having only just started my secondary school, I wasn't socialising as I had done when I was a primary school kid. I lost interest in the football team I’d been fanatical about – Hibernian. I drifted into deep introspection, although I did latch onto different influences. This was the 70s, the era of the Sex Pistols and The Clash who were busy exciting teenage culture. I bought a guitar and started a punk band. I discovered alcohol, the double-edged sword that brought hours of euphoria and confidence, tempered with hangovers and dipping moodswings. I also latched onto Northern Irish politics, draping my bedroom walls in red hand flags. Changing Room - tackling mental health at Hibs and Hearts and beyond Last year I read about a fan initiative being launched at that had been launched at Easter Road stadium, the home ground of my childhood heroes, Hibernian FC. This was called the Changing Room, instigated by the Scottish Association for Mental Health. This outreach initiative as a 12 week programme with one goal: to promote men's mental health and wellbeing through the power of the beautiful game. This hugely successful initiative has since been rolled out to clubs across Scotland, while Scottish Government funding has been provided to launch Changing Room Extra Time sessions to build on the existing programmes, while the Changing Room for Young Women has also been launched at Hibs and Hearts football cubs for women aged 18 to 30. Attitudes to mental health have been evolving steadily since my first psychotic episodes in the 1980s. The situation is never likely to be perfect, but considerable steps have been taken to reduce stigmatisation. This Symposium exemplifies how creative people are continually inspired to seek exciting ways of maintaining positivity and wellbeing.  The Changing Room As someone who has written extensively about a bipolar diagnosis during my 20s prompting three decades of antipsychotic medication, this annual awareness campaign is always poignant. This year I'm fortunate to have benefitted from the support of a mental health outreach programme I joined last October, The Changing Room. Organised by the Scottish Association for Mental Health and piloted at Hibernian FC and then Heart of Midlothian FC in 2018, The Changing Room is a 12-week programme with one goal – to promote men’s mental health and wellbeing through the power of the beautiful game. This hugely successful initiative has since been rolled out to clubs across Scotland, Scottish Government funding has been provided to launch 'Changing Room Extra Time' sessions to build on the existing programmes, while The Changing Room for Young Women has also been launched at Hibs and Hearts for women aged 18 to 30. (Women between the ages of 16 and 24 are almost three times as likely to experience a common mental health issue as males of the same age, 1 in 2 females will stop taking part in any organised physical activity by the age of 20, and around 1 in 5 women have a common mental health problem such as anxiety or depression.) Hibs SOS Participants of the 12-week programmes at Easter Road also have the opportunity to attend monthly drop-ins under the banner Supporting Our Supporters, meeting on the last Monday of every month in the Community Hub at Easter Road, 6-7.30 pm. The main difference to the Changing Room is that the former sessions are delivered by SAMH coaches, whereas the SOS drop-ins are chaired by Hibs Community Foundation (HCF) volunteers who have been through the Changing Room themselves, some of whom have gone on to receive training in coaching by SAMH. 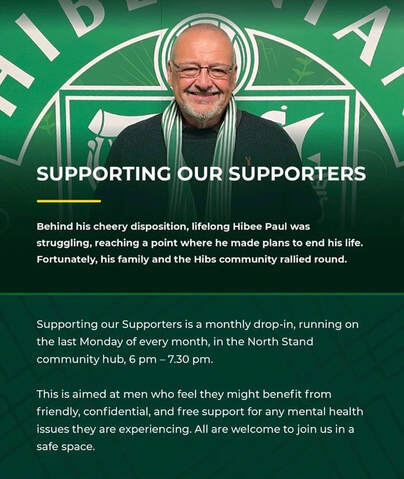 Walk and Talk The opening day of Mental Health Awareness Week, Monday 15 May, coincided with an SOS-arranged 'Walk and Talk.' Pioneered by SAMH, these sessions have become an integral part of the Changing Room programmes, giving participants the opportunity to talk freely about issues they might have side-by-side rather than seated around a table. Against the backdrop of a relaxing stroll around the pitch perimeters of familiar home grounds, participants embark in pairs, discussing the football on their first circuit (sometimes pointing out season ticket seats), relaxing into a mode where they might be more comfortable opening up about their mental health on the next circuit. SAMH organised the inaugural Changing Room 'alumni event' last October, inviting supporters of every Scottish club who'd completed their respective 12-week programmes to the Hampden hospitality suite. As well as touching base with fellow alumni, attendees listened to motivational talks by SAMH and club coaches, and former Hearts, Rangers and Wigan Athletic centre-half, Andy Webster. A key component of this inspirational gathering was a similar chance to 'Walk and Talk' around the national stadium.  At Monday's event, we gained a pitchside view during our 'Walk and Talk,' before retiring to the technical area for a chat. As ever, Lewis Melee, the HCF Head of Community, was on hand to make sure we didn't get locked in! Stories The Changing Room provides a safe environment where participants can share stories. While revealing personal traumas takes courage, open conversations about lived experience of mental health problems can also help others feel more able to talk about their own experiences. Here are some examples from different Changing Room sessions. Neil (Hibs) Ian (Rangers) Robert (Hearts) Gary (Falkirk) Paul (Hibs) Bryan (Hearts) Current Hibernian captain and first goalkeeper David Marshall volunteered to become a member of the HCF Board in 2022. He was a guest speaker at a recent event at the Community Hub, pictured here with HCF/SOS volunteers, Dave Thomson, Neil Renton, Paul Taylor and Mark Fleming.  |

MARK FLEMING EDINBURGH | SCOTLAND
|
 RSS Feed
RSS Feed
